
Last Updated: 12 July, 2015
1.0 Introduction
The heel is a specialised part of the body designed to absorb the impact of your body weight when walking, running or undertaking any other form of physical exertion or weight bearing exercise. An inflamed and irritated plantar fascia can be very painful, therefore when pain does develop, it can be very disabling, making every step a problem which in turn can affect an individual’s overall posture.
From a clinical perspective plantar fasciitis (think pain in the arch of the foot), unfortunately, has the reputation of being a trivial condition clinically, in that it is described as benign and self-limiting (Wolgin et al., 1994; Toomey, 2009) with limited evidence to support any of the common treatments (Crawford & Thomson, 2003; 2010).
However, medical and fitness professionals are starting to appreciate that the greatest public health challenge in Western countries is physical inactivity (Blair, 2009). In this context, plantar fasciitis, which inhibits physical activity due to pain, can be given its due respect (Irving et al., 2008).
Many individuals who develop plantar fasciitis are already overweight (Irving et al., 2006), although the US military states plantar fasciitis is a common problem in soldiers (Morton et al., 2013). Once every day walking becomes painful, the difficulty in losing weight can become problematic and the risk of gaining further weight increases, contributing to a worsening of the condition. Since being inactive and overweight are major risk factors for many diseases, an efficient treatment paradigm for plantar fasciitis – as opposed to a ‘wait and see’ or conservative approach – becomes essential.
Section Two of this overview will provide the reader with a definition of plantar fasciitis, other common terms by which it is known, as well as defining some important terms. Section Three will then provide a description of the foot, particularly the muscles involved. Section Four will outline the causes of plantar fasciitis, why it is a problem and some of the known complications. Section Five will describe who can be affected by the condition and Section Six prevalence and risk factors. Section Seven will look at the symptoms across the identified populations affected by the condition before Section Eight describes how the condition is diagnosed and measured. Section Nine outlines some of the conditions which are similar to plantar fasciitis which the reader should be wary of. Section Ten provides a comprehensive overview of the treatments available such as physiotherapy, exercise and surgical interventions, as well as providing some general advice. Nearing the end, Section Eleven highlights the outlook for people with the condition and Section Twelve provides some summary points of the article. The penultimate section, Section Thirteen, presents opportunity for further reading and finally Section Fourteen provides a full list of references.
2.0 What is Plantar Fasciitis?
Plantar fasciitis can be defined as:
“…a strain of the ligamentous tissues in the bottom of the foot due to chronic overuse, overstretching, and irritation.” (France, 2011, p.365).
The ‘itis’ suffix denotes an inflammatory disorder, which is a misnomer, as the pathology is not a result of excessive inflammation. Pathological changes are degenerative in nature (although partially reversible), presumably due to repetitive micro-trauma. For related tendinopathies, many experts discourage terms such as ‘Achilles tendinitis’ preferring ‘Achilles tendinopathy’ as a diagnosis (Khan et al., 2002).
This debate over terminology has clinical relevance as cortisone injections and anti-inflammatory drugs are contraindicated in some tendinopathies (Coombes et al., 2010) because of the potential for long term weakening of connective tissue.
This concern is of less relevance for plantar fasciitis, as cortisone injections are a treatment modality with moderate supporting evidence (Crawford & Thomson, 2003; 2010). Therefore, there is less of a need to insist on a terminology change.
The fact that the plantar fascia is not a tendon means that successful treatment of the condition can be achieved by strengthening of the enthesis (as one would treat an insertional tendinopathy) or, alternatively, by stretching or even rupturing the medial aspect of the enthesis, which paradoxically can also lead to complete resolution of symptoms (Orchard, 2002).
2.1 Other Terms for Plantar Fasciitis
Plantar fasciitis has gone by a number of different names throughout recent history, which include:
- Heel Spur(s) or Heel Spur Syndrome: Common term but incorrect. A heel spur is another type of issue caused by a calcification on the heel (the spur).
- Plantar Fasciosis (implying that its aetiology is a more chronic degenerative process versus acute inflammation).
- Plantar Fascial Fibromatosis (a condition marked by the presence of or a tendency to develop multiple fibromas).
- Contracture of Plantar Fascia (a permanent shortening (as of muscle, tendon, or scar tissue) producing deformity or distortion).
- Plantar Fasciopathy.
- Subcalcaneal Pain.
- Calcodynia (a condition in which bearing weight on the heel causes pain of varying severity).
- Calcaneodynia (meaning pain in the heel).
- Calcaneal Periostitis (also known as periostalgia, is a medical condition caused by inflammation of the periosteum, a layer of connective tissue that surrounds bone. The condition is generally chronic, and is marked by tenderness and swelling of the bone and an aching pain).
- Painful Heel Syndrome.
- Tennis, Jogger’s, Runner’s or Policeman’s Heel.
As we can see there are a number of alternative terms for plantar fasciitis, however, plantar fasciitis is such a well-established phrase that it will almost certainly remain the preferred term for the clinical syndrome of under-surface heel pain.
To avoid confusion plantar fasciitis is the term used throughout this article.
2.2 Defining the Terms
- Plantar Fasciitis: An inflamed and irritated plantar fascia.
- Fascia: A connective tissue that binds muscles into separate groups.
- Myofascial: The connective tissue in and around muscles and tendons.
- Muscle Imbalance: Alteration of muscle length surrounding a joint.
- Movement Impairment Syndromes: Refer to the state in which the structural integrity of the Human Movement System (HMS) is compromised because the components are out of alignment.
- Lumbo-Pelvic-Hip Complex (LPHC): Involves the anatomical structures of the lumbar, thoracic and cervical spine, the pelvic girdle, and the hip joint.
- Lumbo-Pelvic-Hip Postural Distortion: Altered joint mechanics in an individual which lead to increased lumbar extension and decreased hip extension.
- Lower-Extremity Postural Distortion: Usually characterised by excessive foot pronation (flat feet), increased knee valgus (tibia externally rotated and femur internally rotated and adducted or knock-kneed) and increased movement at the LPHC (extension and/or flexion) during functional movements.
- Flexion: A bending movement where the relative angle between two adjacent segments decreases.
- Dorsiflexion: Flexion at the ankle, moving the front of the foot upward.
- Distal: Refers to a position furthest from the centre of the body or point of reference.
- Dorsal: Refers to a position on the back or towards the back of the body.
- Corrective Exercise: A term used to describe the systematic process of identifying a neuro-musculoskeletal dysfunction, developing a plan of action and implementing an integrated corrective strategy.
- Biomechanics: Applies the principles of physics to quantitatively study how forces interact within a living body.
- Pronation: A multi-planar, synchronised joint motion that occurs with eccentric muscle function.
- Pronation Distortion Syndrome: A dysfunctional muscle pattern characterised by foot pronation and lower extremity muscle imbalances.
- Range of Motion: Refers to the range that the body or bodily segments move during and exercise.
- Tendon: Connective tissue that attaches muscle to bone and provides an anchor for muscles to exert force.
- Tendinopathy: A combination of pain, swelling, and impaired performance commonly associated with the Achilles tendon.
- Tendinosis: Damage to a tendon at a cellular level, but does not present to inflammation.
- Palpation: Physical examination in medical diagnosis by pressure of the hand or fingers to the surface of the body especially to determine the condition (as of size or consistency) of an underlying part or organ.
3.0 Anatomy of the Foot
3.1 Function of the Arches
Although the arch-like structures of the foot are similar to the palmar arches of the hand, the purpose served by each of these systems is quite different. The arches of the hand are structured predominantly to facilitate grasping and manipulation but must also assist the hand in occasional weight-bearing functions.
In contrast, the foot in most individuals is rarely called on to perform any grasping activities. The plantar arches are adapted uniquely to serve two contrasting mobility and stability weight-bearing functions (Van Boerum & Sangeorzan, 2003). First, the foot must accept weight during early stance phase and adapt to various surface shapes:
- To accomplish this weight-bearing mobility function, the plantar arches must be flexible enough to allow the foot to:
- Dampen the impact of weight-bearing forces;
- Dampen superimposed rotational motions; and
- Adapt to changes in the supporting surface.
- To accomplish weight-bearing stability functions, the arches must allow:
- Distribution of weight through the foot for proper weight-bearing; and
- Conversion of the flexible foot to a rigid lever.
The mobility-stability functions of the arches of the weight-bearing foot may be examined by looking at the role of the plantar aponeurosis and by looking at the distribution of weight through the foot in different activities.
3.2 Plantar Fascia
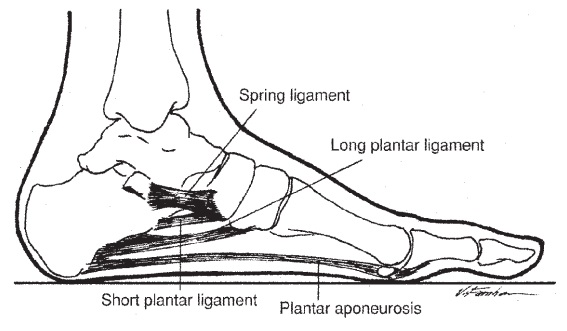
The plantar fascia (or plantar aponeurosis) is a dense fascia (a strong layer of white fibrous) that runs nearly the entire length of the sole of foot (Figure 1). It begins posteriorly on the medial tubercle of the calcaneus and continues anteriorly to attach by digitations to the plantar plates and then, via the plates, to the proximal phalanx of each toe. From the beginning to the end of the stance phase of gait, tension on the plantar fascia increases, with maximum tension averaging 96% of body weight as force is transmitted from the Achilles tendon to the forefoot (Erdemir et al., 2004).
Towards the front of the foot, at the mid-metatarsal level, it divides into five sections, each extending into a toe and straddling the flexor tendons. Laterally, it is divided into three sections:
- Medial: The medial portion overlies the muscles to the hallux (big toe).
- Lateral: The lateral portion overlies muscles to the little toe.
- Central: Is designated as the plantar fascia. It is the most important structurally and functionally, and is attached at its origin to the medial calcaneus (heel bone).

The plantar fascia supports the longitudinal arch of the foot with a similar function as the bowstring of a bow or windlass (De Garceau et al., 2003). During walking, the plantar fascia functions mainly during ‘heel rise’ to ‘toe off.’ It stabilises the arch of the foot and allows flexion of the first metatarsal, enabling the first metatarsal to carry the majority of the body weight. It also provides shock absorption when the foot hits the ground. All three components of the plantar fascia arise from the plantar tubercle of the calcaneus. This segment of the plantar fascia is prone to degeneration or discrete tear.
Plantar fasciitis is a chronic, recurrent, and frequently debilitating condition. The fascia may be thickened, with areas of nodularity in chronic cases. In acute fasciitis, there may be soft tissue oedema adjacent to a normal-thickness plantar fascia. Plantar fasciitis occurs at the proximal attachment and is an enthesopathy, the enthesis being the interface between the bony surface (periosteal) and a tendon or ligament attachment. Most tendinopathies (such as tennis elbow) are insertional, and hence also enthesopathies.
The plantar fascia is a ligament in anatomical terms (Madden et al., 2010), because it attaches bone to bone (calcaneus to metatarsal heads, crossing other joints of the foot in its path, Figure 2) rather than a tendon (which attaches muscle to bone).
However, deep to the superficial structure of the plantar fascia is the flexor digitorum brevis muscle, with a tendon enthesis attachment to the calcaneus proximally. As stress shielding (failure of a stress deprived deep surface to heal because the superficial element bears most of the load) is potentially implicated in enthesopathy (Orchard et al., 2004), it is possible that proximal tendinopathy of the flexor digitorum brevis muscle is involved in the pathology of plantar fasciitis.
4.0 What Can Cause Plantar Fasciitis?
Madden and colleagues (2010, p.465) describe the aetiology of plantar fasciitis as” Excessive tightness of gastrocsoleus complex pulling into Achilles tendon causes overload at plantar fascia origin on calcaneus during weight-bearing activities; micro-tears and inflammation ensue.”
Kisner and Colby (2012, p.868) suggest that “Pressure transmitted to the irritated site with weight bearing or stretch forces to the fascia, as when extending the toes during push-off, causes pain. A heel spur may develop at the site of irritation on the calcaneus, causing pain whenever the heel is on the ground.”
The general consensus has moved away from inflammation as the cause to microtears in the origin of the plantar fascia, leading to inflammation.
With this in mind, plantar fasciitis can be caused by a number of factors as outlined below:
- A sudden increase in training mileage;
- Poor shoes or inappropriate footwear (Kisner & Colby, 2012);
- Training surface problems;
- A single severe training session;
- Dynamic Malalignment (specifically “lower extremity movement impairment syndrome”) (Clark & Lucett, 2011, p.66-68);
- Distal Injuries: “because of the connectivity of the structures and tissues of the kinetic chain, dysfunction can migrate toward or stem from imbalance or injury from other areas of the body.” (Clark & Lucett, 2011, p.323);
- Lack of ankle dorsiflexion (Irving et al., 2006; McPoil et al., 2008), believed to be associated with rather than a cause of, viewpoint dependent on the research you read;
- In court sports athletes it is “Caused by repetitive pushing off and jumping.” (Madden et al., 2010, p.504); and
- Pronated foot type (Irving et al., 2007; Clark & Lucett, 2011);
It is often noted that some change in activity level (i.e. increase) occurred before the onset of pain!
Plantar fasciitis can be an acute or chronic condition.
4.1 Why is it a Problem?
The plantar fascia has been shown to contribute to numerous components of stance and gait, including support of weight bearing, propulsion, shock absorption and adaptation to uneven ground (Norkin & Levangie, 2001).
Plantar fasciitis is a problem because when pain develops it can be very disabling, making every step a problem which in turn can affect an individual’s overall posture and impact on an individual’s ability or desire to undertake physical activity or exercise.
As such, those affected by plantar fasciitis should be concerned about the functional issues of having the condition which may have a significant impact on their daily activities, noting that:
- Individuals often limp, place the body weight on the toes, or try to avoid walking on the affected foot.
- Individuals may adjust the way they walk or run in order to avoid knee, hip, back, and other foot pain.
- The condition may prevent individuals from bending the foot, causing the toes to point upwards toward the shins, which may be painful.
- Individuals may also be unable to bend the foot, resulting in decreased flexibility.
When conducting activities such as going up stairs, exercise, or other acts of daily living, plantar fasciitis can cause other parts of the body, such as the LPHC, to work harder. Therefore, cure/repair of the plantar fascia (through manual therapy or surgery) often gives individuals better use of the lower body, and often improves other associated symptoms if they are present.
4.2 What are the Complications?
It is important to note that this condition has associated morbidity but no associated mortality . Some researchers suggest that failure to treat plantar fasciitis successfully can lead to long term sequelae , including:
- Limited physical activity or exercise capability.
- Limited normal daily activities.
- Abnormal or poor postural stability.
- Physical discomfort, such as low back pain or lumbo-pelvic pain.
- Lateral plantar nerve injury.
- Complete release of the plantar fascia with destabilisation of medial longitudinal arch.
- Increased stress on the dorsolateral mid-foot.
- Chronic pain.
- Plantar fascia rupture: Complications may also arise from treatment selection (corticosteroid injections and surgical procedures may cause the fascia to rupture or tear and worsen symptoms, such as pain and weakness). Risk factors are athletes, minimalist runners and/or corticosteroid injections, and is treated with cast immobilisation.
There is a general consensus that medical professionals may not take plantar fasciitis seriously as it has the reputation of being a trivial condition clinically, in that it is described as benign and self-limiting (Wolgin et al., 1994; Toomey, 2009). Plantar fasciitis does not lead to emergency conditions, but symptoms can develop in the long-term perspective due to distal injury or postural changes.
5.0 Who Can Be Affected By Plantar Fasciitis?
Although plantar fasciitis can occur in both genders and across age groups, it is principally seen in middle aged or older people. Populations affected include:
- Older Population: Typically, middle aged and older people are affected more than other population groups (Scher et al., 2009). Along the plantar aspect of the heel, atrophy of the fat pad begins after 40 years (Pfeffer, 2001). A gradual age-related loss of collagen, water, elastic fibres, and overall volume of the fat pad is attributed to creating a softer and thinner pad less equipped to dissipate load-bearing forces (Ozdemir et al., 2004).
- Female Population: women slightly more often than men (Scher et al., 2009).
- Running Population: typically irregular or minimalist runners.
- Athletic Population: Athletes can get plantar fasciitis, but not as often as other overuse injuries such as tendinopathies and stress fractures.
- Higher BMI Population: Increased BMI (body mass index) in a nonathletic population has also been indicated as a predisposing factor (McPoil et al., 2008; Kisner & Colby, 2012).
6.0 Prevalence and Risk Factors
With regards to prevalence Riddle and colleagues (2004) conducted research to generate (US) national estimates of the volume of patient visits and characteristics of care given to patients diagnosed with plantar fasciitis by medical doctors. They found:
- Approximately 1 million patient visits per year were made to office-based physicians and hospital outpatient departments for the diagnosis and treatment of plantar fasciitis during 1995-2000.
- Approximately 62% of all visits were made to primary care practitioners, and 31% were made to orthopaedic surgeons.
- Patient visits for plantar fasciitis accounted for approximately 1% of all patient visits to orthopaedic surgeons.
- Pain medication, including non-steroidal anti-inflammatory drugs (NSAIDs), was the most frequently used intervention (47% of visits).
- Exercise counselling was cited at 26% of visits, and physical therapy was ordered or provided at 19% of visits.
Riddle and colleagues (2004) went on to conclude that plantar fasciitis was a relatively common disorder, seen by several physician specialties, but was not managed in a consistent way. They also suggested there appeared to be a large amount of variation in the way that patients were managed and argued that additional research was needed to identify effective/optimal interventions for plantar fasciitis; something that has not necessarily changed (Orchard, 2012; Sullivan et al., 2015).
The wisdom in the literature suggests there are a number of risk factors for developing plantar fasciitis, which include:
- Those who walk a lot, particularly at work, are more at risk (Riddle et al., 2003), which is reflected in a lay term for the condition, “policeman’s heel.”
- Increased body weight is a well-established risk factor, BMI (body mass index) >30 kg/m2 (Irving et al., 2006; Riddle et al., 2003; Sullivan et al., 2015).
- There is some evidence that work on hard surfaces increases the risk (Werner et al., 2010).
- Court sport athletes (who compete on hard surfaces) seem to have greater risk than footballers and others who play on softer surfaces such as grass.
- Reduced range or lack of ankle dorsiflexion (tightness of the foot and calf musculature), in a non-athletic population, is associated with plantar fasciitis (Irving et al., 2006; McPoil et al., 2008), as are calf and hamstring tightness (Labovitz et al., 2011).
- Decreased and increased range of ankle dorsiflexion range of movement (Bahr & Engebretsen, 2009; Sullivan et al., 2015). The risk of plantar fasciitis increases as the range of ankle dorsiflexion decreases (Riddle et al., 2003).
- Reduced ankle dorsiflexion, obesity, and work-related weight-bearing appear to be independent risk factors for plantar fasciitis. Reduced ankle dorsiflexion appears to be the most important risk factor (Riddle et al., 2003).
- Reduced ankle evertor and toe flexor strength, and an altered inversion/eversion strength ratio (Sullivan et al., 2015).
- In a clinical survey of runners’ injuries by James and colleagues (1978), plantar fasciitis was one of five diagnoses associated with pronation, the others being chondromalacia, knee pain, Achilles tendinitis and posterior tibial syndrome. James emphasized, however, that no single anatomic variation correlated with any specific diagnosis.
- Pronated foot type (Irving et al., 2007) or “overpronation (foot rotating inward) can cause several problems with the lower leg, including plantar fasciitis” (France, 2011, p.236).
- Pronation Distortion Syndrome (Clark and Lucett, 2011): Individuals with pronation distortion syndrome develop predictable patterns of injury, including plantar fasciitis, posterior tibialis tendinitis (shin splints), patellar tendonitis, and low back pain (Kaufman et al., 1999; Irving et al., 2007; Kaufman et al., 1999; Moen et al., 2009).
- In 202 people with plantar heel pain and 70 asymptomatic control participants there were no differences between the two groups for foot alignment, dorsiflexor or invertor strength, ankle inversion or eversion range of motion, first MTP joint extension range of motion, generalised hypermobility, occupational standing time, or exercise level (Sullivan et al., 2015).
- Some researchers suggest that there is not strong evidence to associate foot type or first metatarsophalangeal joint motion with plantar fasciitis (Irving et al., 2006; Irving et al., 2007).
- “…a flexible flat foot (pes planus) may be predisposing factors. Conversely, stress forces on the fascia also may occur with an excessively high arch (cavus foot).” (Kisner & Colby, 2012, p.868).
- “Seen in both pes planus and pes cavus, although latter more common. Tight gastrocnemius-soleus complex and plantar flexors as well as excessive pronation increase risk of developing plantar fasciitis.” (Madden et al., 2010, p.561).
- “Plantar fasciitis is a common injury that can stem from Lower-Pelvic-Hip Complex (LPHC) dysfunction.” (Clark & Lucett, 2011, p.292).
- Weight bearing endurance activity (e.g. dancing or running).
- Associated impairments include hypo-mobile gastrocnemius-soleus muscles and plantar fascia pain or restriction when extending the toes creating the windlass effect (Kisner & Colby, 2012).
- Inappropriate footwear (Kisner & Colby, 2012).
- Human leucocyte antigen (HLA) B27 associated spondyloarthropathies. Includes psoriatic and reactive arthritis and is commonly accompanied by bilateral plantar fasciitis, which confers a poorer prognosis for resolution.
- Evidence of an occupational link is sparse, and plantar fasciitis is not recognised as a work-related or industrial injury.
- Within a US military cohort risk factors include: female sex; black race; junior enlisted, senior enlisted, and senior officer rank groups; service in the Army or Marines; and increasing age (Scher et al. 2009).
7.0 What are the Symptoms?
With plantar fasciitis, there are no visible features on the heel but a deep localised painful spot found in or around the middle of the sole of the heel will be very tender to palpation (i.e. touch) (Kisner & Colby, 2012).
Individual’s will feel an insidious onset of heel pain/point tenderness (particularly on first step in morning), specifically where the plantar fascia inserts on the medial tubercle of the calcaneus (Kisner & Colby, 2012), and may prefer to walk on their toes initially. Pain is sometimes relieved with ambulation (i.e. movement), although returning after rest (known as start-up pain) (McPoil et al., 2008; Madden et al., 2010; Thomas et al., 2010).
The pain can be worse at the end of the day after prolonged standing and it is common to have symptoms bilaterally (i.e. both heels) and individuals will usually avoid “heel-strike during the loading response of gait” (Kisner & Colby, 2012, p.868).
It is estimated that around 10% of the population have plantar fasciitis without any pain whatsoever.
8.0 How Is Plantar Fasciitis Diagnosed?
Plantar fasciitis should only be diagnosed by an appropriately qualified professional (e.g. a physiotherapist, podiatrist/chiropodist or medical doctor) who will check for the condition by inspecting the affected area.
With this in mind, plantar fasciitis can be diagnosed through a number of methods as outlined in Table 1.

- Foot & Ankle Ability Measure (FAAM)
- Foot Function Index (FFI)
- Foot Health Status Questionnaire (FHSQ)
- Visual Analogue Scale (VAS)
8.1 Palpation
Palpation of the hind-foot includes careful evaluation of the calcaneus. Along the medial calcaneal tubercle arises the origin of the plantar fascia. Plantar fasciitis or fasciopathy is a common painful condition. A classic historical clue is heel pain that is worse with the first step in the morning. The examiner should take care to evaluate the origin of the plantar fascia as well as the proximal fibres. Areas of tenderness, abnormal thickening, and possible defects should be noted and compared to the unaffected side. In cases of severe or prolonged plantar fasciitis, the origin on the calcaneus may become oedematous (an abnormal excess accumulation of serous fluid in connective tissue) and painful as well.
The experienced clinician will also note that not all heel pain is derived from plantar fasciitis. The calcaneus is one of the strongest bones in the body but it still may develop stress injury. The examiner can cup the heel between their palms and apply a gentle squeezing force across the calcaneus. Significant pain in the calcaneus with this test should prompt concern for stress reaction or fracture even if plain film radiographs are normal. The individual should then be referred for an advanced imaging and placed on crutches (Philbin, 2014).
When utilising neural testing and mobilisation techniques for the lower quadrant, for example the sciatic nerve (straight-leg raising with ankle dorsiflexion), changing positions of the ankle in conjunction with variations in the hip and knee positions are used to differentiate foot impairments, such as plantar fasciitis and tarsal tunnel syndrome (Alshami et al., 2008).
8.2 Diagnostic Imaging

Although diagnostic imaging can be used in the clinical management of plantar fasciitis, it does not commonly change management (Orchard, 2012). Many authors have established that, although the diagnostic imaging features of plantar fasciitis (such as heel spur on x ray (Figure 3) (Irving et al., 2006) thickened plantar fascia on ultrasound (Akfirat et al., 2003), and “hot” bone scan on calcaneus) are far more common in patients with heel pain, they can occur in asymptomatic individuals and be absent in cases of plantar fasciitis.
It is recognised that the pain is not simply due to a heel spur, although the exact cause of pain in plantar fasciitis (and other enthesopathies) remains uncertain (Orchard, 2012). Where the diagnosis is unclear from the standard clinical assessment, pain relief on walking after an ultrasound guided injection of local anaesthetic to the plantar fascia origin can help to confirm the diagnosis (Orchard, 2002).
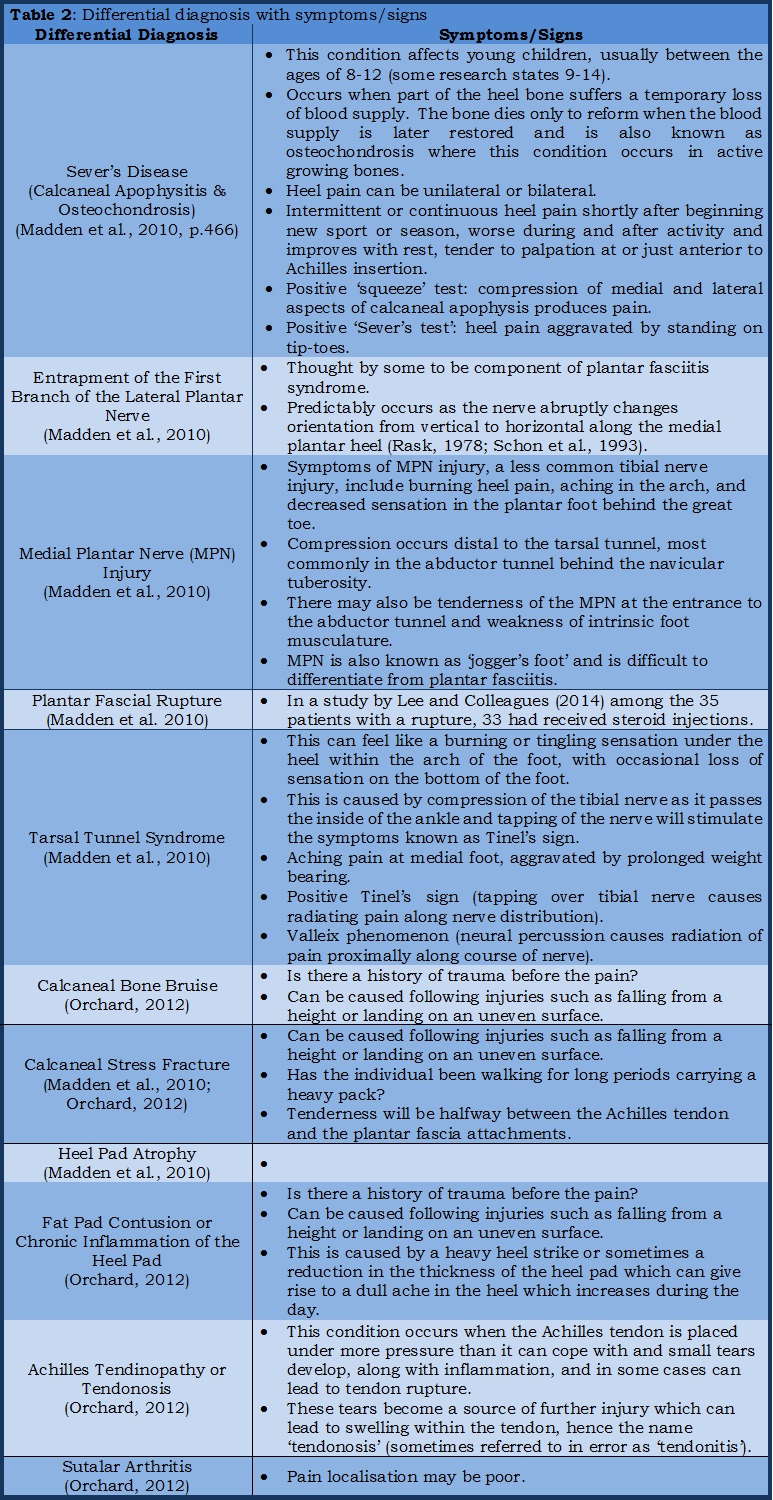
9.0 Differential Diagnosis

Heel pain can sometimes represent a diagnostic challenge, but most of the time the diagnosis of plantar fasciitis is straightforward, with the challenge being one of successful management (Orchard, 2012). Achilles tendinopathy, the other common cause of chronic heel pain of gradual onset, is differentiated by location – on the posterosuperior aspect of the heel as opposed to the under-surface, where plantar fasciitis occurs, typically on the medial aspect of the under-surface (Figure 4). In general, the tenderness of heel pain localises well, which confirms the diagnosis of plantar fasciitis or Achilles tendinopathy. In cases where pain localisation is poor, a differential diagnosis needs to be considered (such as subtalar arthritis or S1 nerve root impingement (Neve et al., 2010)). If there is a history of trauma before the pain (such as landing on the heel from a height), other diagnoses, such as fat pad contusion or calcaneal bone bruise, need to be considered. Calcaneal stress fractures are uncommon, but they can be suspected in cases where the patient has walked for a long period carrying a heavy pack. Runners tend to get stress fractures in bones other than the calcaneus, because compared with walking, relatively less of the gait cycle is spent bearing weight through the heel. Tenderness in a case of stress fracture will be halfway between the Achilles tendon and plantar fascia attachments (seen in Figure 4).
The following types of heel pain (described in Table 2 and sub-Section 9.1 to 9.4) are not exhaustive but may help you appreciate the complexity of heel pain and why specialist advice can be helpful.
9.1 Calcaneal Stress Fractures
Calcaneal stress fractures are considered low risk stress fractures due to their ability to heal and low likelihood of progression to complete fracture. In a study of military recruits, they accounted for 28% of stress fractures (Wilson & Katz, 1969). Unfortunately, these are frequently misdiagnosed as plantar fasciitis or Achilles tendinitis, with treatment frequently delayed. Most commonly, this fracture occurs in individuals after a significant increase in training volume or intensity; they are most common in distance runners.
Unlike plantar fasciitis, the pain associated with stress fracture is typically present throughout the day and is worse with activity. Swelling is usually minimal. The individual will be tender to compression of the calcaneal tuberosity. Radiographically, a sclerotic line may be seen running perpendicular to the trabeculae of the calcaneus, although often a nuclear medicine scan or MRI is needed to confirm the diagnosis. Treatment typically consists of activity modification. Frequently the individual is placed into a controlled ankle motion walker initially to decrease the tension on the tuberosity from the pull of the Achilles tendon. The individual is permitted to bear weight as tolerated and gradually wean from the boot and progress activities as pain allows. Frequently this requires 6-8 weeks of treatment. “If activity is resumed too quickly, the pain typically recurs requiring an additional period of inactivity.” (Philbin, 2014, p.122-123).
9.2 Heel Bursitis (Subcalcaneal Bursitis)
This is an inflammation of a bursa (a fluid filled fibrous sac) under the heel bone where the pain is typically more in the centre of the heel than that experienced with plantar fasciitis and significantly worsens during the day. This condition can be caused following a fall from a height on to the heel.
With heel bursitis, pain can be felt at the back of the heel when the ankle joint is moved and there may be a swelling on both sides of the Achilles tendon, or feel pain deep inside the heel when it makes contact with the ground.
9.3 Heel Bumps
These are firm bumps on the back of the heel and these are usually caused by excessive shoe rubbing in the heel area.
9.4 Associated Conditions/Disorders
There are a number of other associated conditions/disorders that should be noted:
- Gastrocnemius-soleus Contracture;
- Heel Pain Triad;
- Posterior Tibial Tendon Dysfunction;
- Anatomic variations;
- Pes Cavus: A high medial arch when weight bearing;
- Pes Plantus: A flattened medial arch during weight bearing;
- Morton’s Neuroma (occurs at the ball of the foot and toes);
- Gout;
- Reiter’s syndrome; and
- Dupuytren’s contracture causes similar swelling of the plantar fascia but this condition is usually painless.
10.0 Treatment
Many systematic reviews of plantar fasciitis management have been performed, with a common finding that high quality evidence of efficacy for any one treatment modality is lacking (Crawford & Thomson, 2003; 2010). However, the situation in specialist clinical practice is not nearly as bleak as the systematic reviews would suggest, with multiple treatment modalities well described and many with low or moderate level evidence (Cole et al., 2005; Thomas et al., 2010). All of the common treatment modalities have a place, yet all of them will be unsuccessful for some individuals; although it must be noted that 90% of patients will improve with conservative therapies (Donley et al., 2007; Thomas et al., 2010).
The essence of good clinical practice is to provide a benefit-risk equation for the common treatments and to tailor the best treatment for a particular individual, taking into account the unique circumstances. Importantly, the condition should not be trivialised, as the holistic cost to the individual – particularly if they are overweight – of a prolonged period of finding everyday walking painful is high. Therefore, low or moderate cost treatments with a fair chance of success should be attempted, as the potential general health gain of return to pain-free walking is high. When a treatment modality has been identified Madden and colleagues (2010, p.466) suggest that “Early intervention [is] more efficacious than late intervention.”
10.1 Prevention and General Advice
Prior to moving on to discuss the general treatment modalities available for plantar fasciitis, it is wise to note that prevention is better than cure. With this in mind Madden and colleagues (2010, p.553) suggest developing “…smaller supporting muscles. Strengthening prevents development of shin splints, plantar fasciitis, patellofemoral dysfunction, and other overuse injuries.”
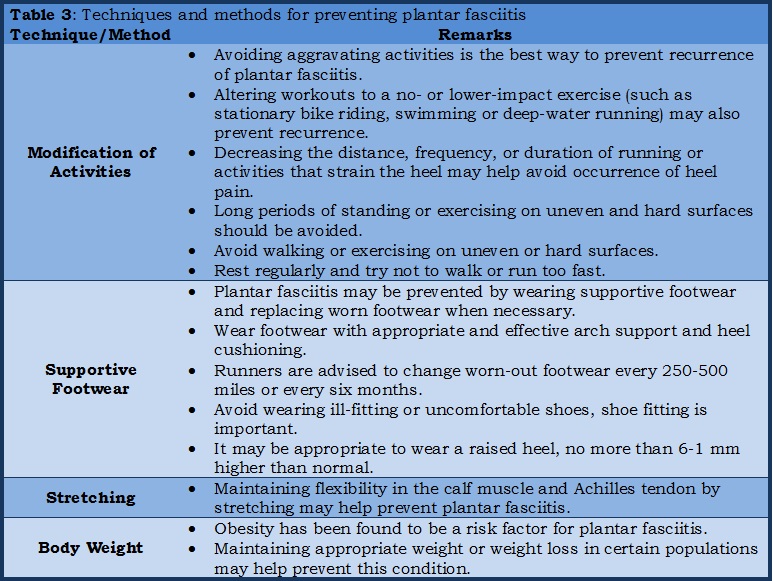
Some techniques and methods for preventing plantar fasciitis, with general advice, is outlined in Table 3.
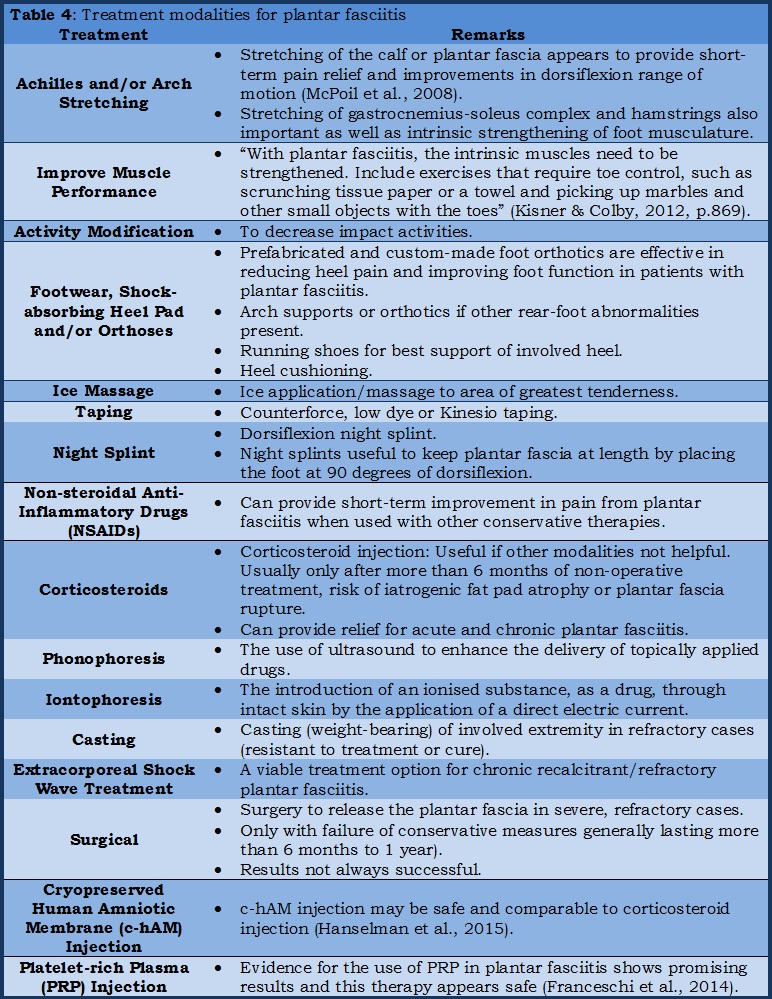
10.2 Treatment Modalities
Treatment can take many forms (Table 4) from resting your foot as much as possible, stretching exercises and deep heat therapy to steroid injections and even medication or surgery to release the tight tissue ‘band’. In some cases, padding and strapping is applied to alter the direction of stretch of the ligament to alleviate symptoms in the short-term. However, for the long-term, special insoles (orthoses) are prescribed to help the feet to function more effectively and help to make any possible recurrence less likely.
Consistently the major categories of treatment recommended, assessed, or reviewed in studies were:
- Biomechanical treatment, including orthotics, other footwear modification, and taping;
- Stretching techniques, particularly including night splints;
- Extracorporeal shock wave therapy;
- Cortisone (or other) injections; and
- Surgery.
Although other treatments are available and described, these categories cover what most experts would consider to be the established treatments for plantar fasciitis. They are all consistently described as having some role in management, but no review has established that a particular treatment has the highest level of evidence (that is, consistently superior results to placebo in high quality randomised controlled trials). Based on analysis of research, expert consensus suggests treatment options should be offered to the individual in sequence, based on either:
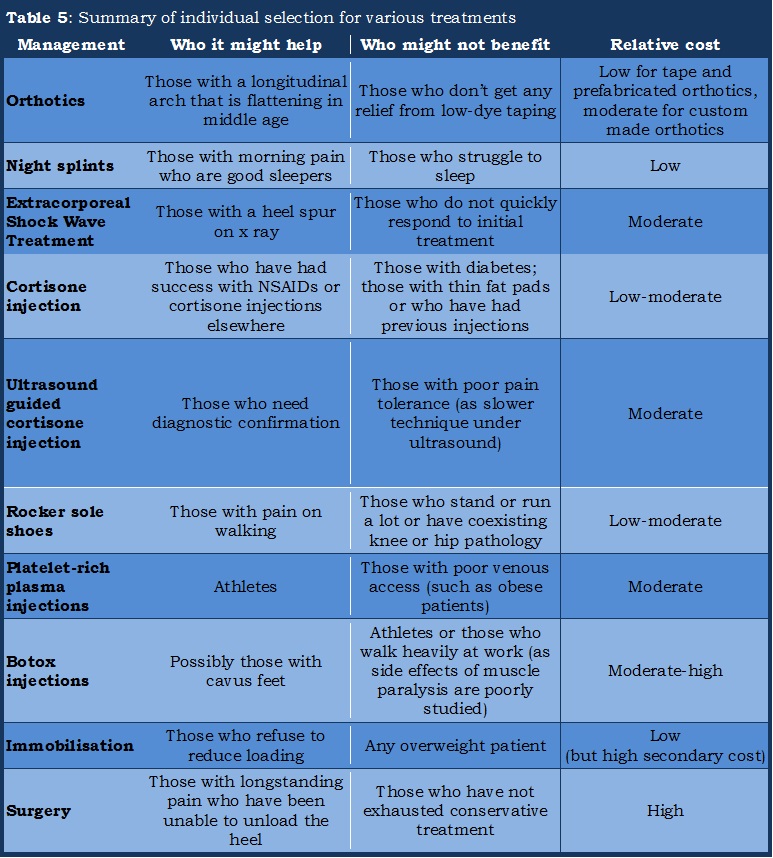
- Objective criteria that may predict who would respond best to each treatment modality (see Table 5); or
- Patient preference, as compliance with treatment is likely to be associated with success and common sense would dictate that patients are most likely to comply with their preferred treatment.
In most cases it is sensible to offer isolated treatment modalities so that response can be assessed.
10.3 Orthotics, Taping and Footwear Modifications

Perhaps the most common group of treatments for plantar fasciitis is footwear modifications, including orthotic devices (prefabricated or custom made, Figure 5). Although there is no strong evidence that orthotics are effective for all cases of plantar fasciitis (Landorf et al., 2006), analysis of pooled papers suggest moderate improvements (Lee et al., 2009). Cost effectiveness of custom made orthotics is not well established, as they are moderately expensive and have not been shown in trials to be superior to cheaper prefabricated orthotics (Landorf et al., 2006). However, custom made orthotics are more durable and are likely to be better tolerated because of their specific fitting.

Orthotic devices, theoretically, reduce pronation and thereby unload the plantar fascia. This is also the suggested mechanism of action for low-dye taping (Figure 6), which also has limited evidence (Van de Water & Speksnijder, 2010). Because of the moderate expense of custom made orthotics and their variable efficacy, it is suggested that they are not prescribed routinely but are used in cases where individuals report improvement with prefabricated orthotics or low-dye taping. Kinesiotaping, involving both calf and foot, may work in a similar fashion (Tsai et al., 2010).

Biomechanical teaching would also suggest that orthotics are more likely to be successful in individuals with flat feet (who over-pronate). Practical considerations mean that orthotics will be less helpful and less likely to be tolerated by individuals who prefer to wear open or tight fitting shoes. Paradoxically, women often report less pain from plantar fasciitis when wearing high heeled shoes, yet regular wearing of high heels is blamed for the development of a shortened plantar fascia, making the condition more likely (Orchard, 2012).
Another footwear modification that has the potential to help some patients is the rocker-sole shoe (Figure 7) (Janisse & Janisse, 2008). Patients should be warned that these shoes lead to poorer balance and can potentially aggravate knee, hip, and low back problems. However, as the weight bearing is more through the mid-foot and less through the heel and toe, they can be valuable, for example, for patients who walk regularly at work.
10.4 Stretching and Night Splints
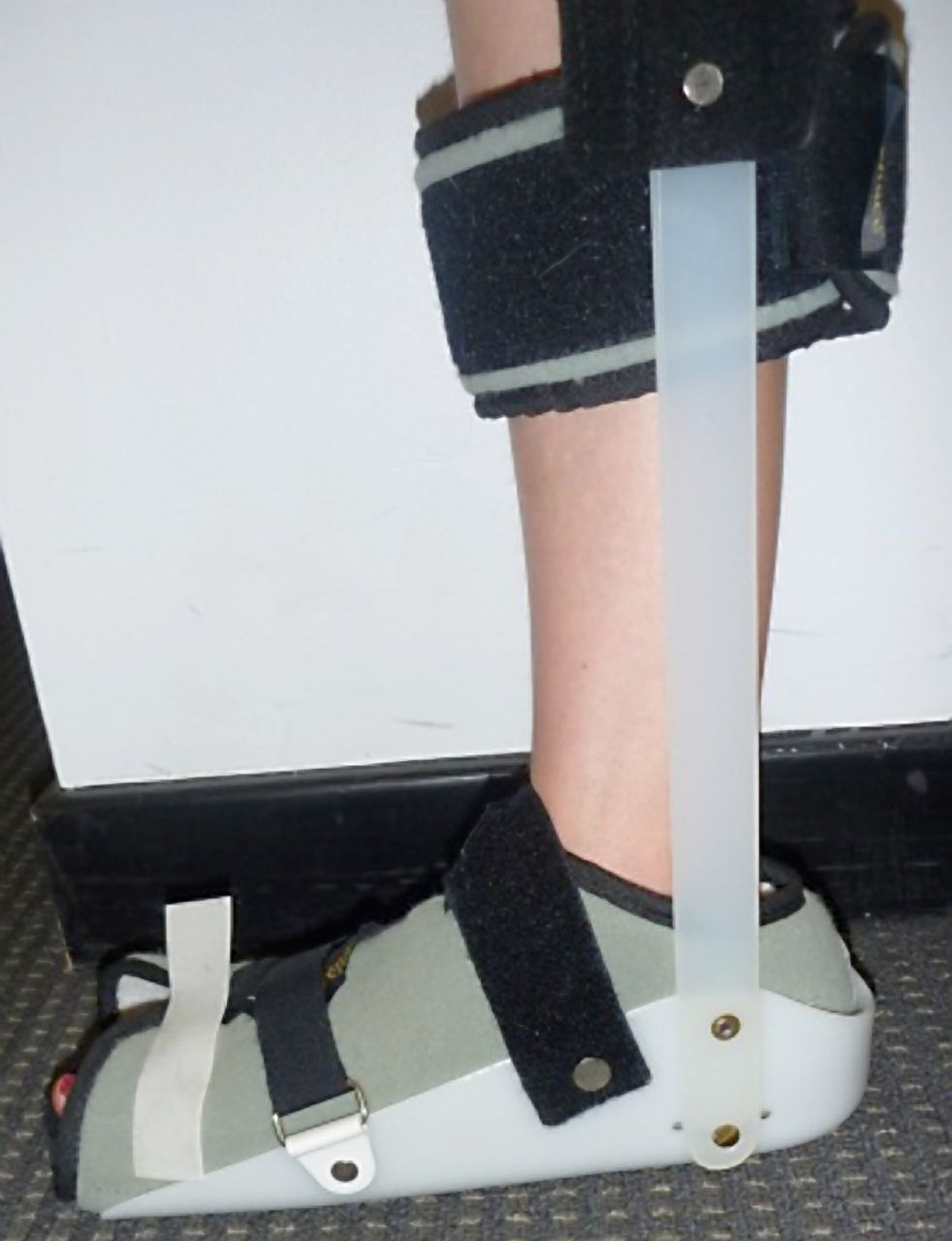
Stretching has been shown to provide some help in plantar fasciitis (DiGiovanni et al., 2006), although it is arduous treatment with limited success. Stretching can be performed against a solid object or by using a hard object such as ball or bottle. A night splint (whether rigid (Figure 8) or a ‘sock’) can, in theory, provide a stretch lasting for many hours, with the potential for greater effect (Barry et al., 2002). Compliance is the major argument against a trial of night splints (Roos et al., 2006). Poor sleepers would probably be wasting their time if they tried to use one of these devices, as they certainly do not promote a good night’s rest. However, for those who tolerate them, they are a good, low risk, non-invasive option. They seem to be particularly good for those patients with severe pain on getting up in the morning. Stretches themselves are of use and should be encouraged for most patients.
10.5 Extracorporeal Shock Wave Therapy

Extracorporeal shock wave therapy is a well-established treatment for kidney stones and was initially trialled in the management of plantar fasciitis because the x ray appearance of a calcaneal spur was similar to that of a renal calculus. There have been many randomised controlled trials of shock wave therapy for treating plantar fasciitis, making it the most researched modality, but the results have been somewhat inconclusive (Rompe et al., 2007). A 2007 review analysed 17 controlled trials as having mixed but generally positive results (Rompe et al., 2007) with further encouraging subsequent publications (Metzner et al., 2010; Othman & Ragab, 2010) and support from recent meta-analysis (Chang et al., 2012). Most, but not all, individuals will tolerate the therapy (Figure 9) without anaesthetic because of the attenuation of shock from the fat pad. It has still not been determined whether the shock is best aimed at the calcaneal spur, if present, or at the area of maximum tenderness. Although no comparison has been made of results in individuals with and without calcaneal spur, since shock wave therapy tends to work only for tendinopathies with calcific change, it would be more advised in individuals with an obvious spur on x ray.
10.6 Cortisone (including Iontophoresis) and Other Injections
Cortisone injections are the most common ‘medical’ treatment used for plantar fasciitis. They have evidence of efficacy in the short term, with some trials showing greater response than other treatments (Porter & Shadbolt, 2005). However, because cortisone has greater side effects than modalities such as extracorporeal shock wave therapy, it can equally be argued that the cheaper (cortisone injection) or less invasive treatment (shock wave) should be used initially (Yucel et al., 2010).
One comparison study suggested that if ultrasonography revealed perifascial oedema then cortisone injections gave superior results, but if not, then shock wave therapy gave superior results (Sorrentino et al., 2008). Cortisone iontophoresis has also been used, for those who wish to avoid the pain of an injection (Peplinski & Irwin, 2010). Injections are notoriously painful, particularly when ultrasound guided (as the procedure takes longer), although it is argued that ultrasound guided injections are more accurate (Tsai et al., 2006; Tatli & Kapasi, 2009). Non-guided injections can be performed more rapidly, but there is risk of depositing the cortisone into the fat pad, with fat pad wasting a potential complication of these injections. Another approach is to try to reduce the pain of injection with a median calcaneal nerve block.
It is quite plausible (because plantar fasciitis is considered an enthesopathy but not a tendinopathy) that cortisone injections are more successful in plantar fasciitis than tendinopathies. It is also possible that studies of cortisone injections in plantar fasciitis have not generally reported long enough follow-up to reveal a reversal of initially good results (Coombes et al., 2010). In other enthesopathies (such as tennis elbow) there has been a shift towards the use of newer injection options such as platelet rich Plasma (Coombes et al., 2010; Peerbooms et al., 2010a). The only comparative study to date showed no difference in effectiveness between platelet rich plasma and cortisone for plantar fasciitis (Aksahin et al., 2012), although a larger trial is underway (Peerbooms et al., 2010b).
At least three trials have shown a potential role for botulinum toxin injections in plantar fasciitis (Babcock et al., 2005; Placzek et al., 2005; Huang et al., 2010). If further high quality study confirms a benefit, it will suggest that flexor digitorum brevis tendinopathy is part of the plantar fasciitis pathology, as a muscle toxin can theoretically have an effect only on a tendon (by relieving muscular pulling) rather than the ligament component of the plantar insertion.
However, Lee and Colleagues (2014) suggest that steroid injections for plantar fasciitis should be cautiously administered because of the higher risk for plantar fascia rupture.
10.7 Surgery
Surgery remains an option for longstanding cases of plantar fasciitis, with case series evidence of success (Bazaz & Ferkel, 2007; Marafko, 2007; Sinnaeve et al., 2008; Maskill et al, 2010). As with many other musculoskeletal conditions, there is no evidence from randomised control trials to support surgery. Given that the prognosis for most cases is benign, it is hard to justify surgery in a case of only a few months’ duration given the likely success with less invasive methods. The fact that rupture of the plantar fascia has been reported to sometimes cure the condition (Orchard, 2002) suggests that surgical division of the origin (performed with open or arthroscopic technique) might give success in resistant cases. Although hamstring and calf tightness are associated with plantar fasciitis (Labovitz et al., 2011), cause and effect has not been proved, and it may be that these phenomena are all caused by subtle L5 and S1 nerve impingement in older people (Orchard et al., 2004). Good results obtained from gastrocnemius release in plantar fasciitis (Maskill et al., 2010; Abbassian et al., 2012) either supports a role for aetiology or suggests that much of the success of surgery may be due to a prolonged period of unloading and reloading.
10.8 Weight Loss in Plantar Fasciitis
Weight loss can be particularly problematic in plantar fasciitis, as one of the primary components of a sensible weight loss programme (less sitting, more standing and walking) can be compromised by the pain of plantar fasciitis.
Cross training (such as swimming and cycling) can be particularly valuable until the pain starts to resolve.
Although it is not covered in the literature as a plantar fasciitis treatment, tracking daily step counts with pedometers can be useful in the management of plantar fasciitis – initially to unload, and then to manage return to higher loads. Pedometers are currently the most common method for managing step counts (and hence loads), but they are likely to be superseded soon by global positioning system (GPS) and accelerometer technology in mobile phones which could equally record steps per day.
10.9 Podiatrists and Chiropodists
Podiatrists can be thought of as a type of foot doctor, as they can give individuals advice on how to look after their feet, what type of shoes to wear, and also supply orthotics, which are tailor-made insoles, padding and arch supports to relieve arch or heel pain.
Podiatrists work in the NHS and private practice, in both cases, always ensure that any practitioners you visit are registered with the Health Professionals Council (HPC) and describe themselves as a podiatrist (or chiropodist). To contact an NHS podiatrist individuals will need to contact their GP for an NHS referral, although in some areas you can self-refer.
There is no difference between a podiatrist and chiropodist, podiatrist is simply a more modern name.
11.0 What is the Prognosis or Outlook?
There are no treatments for plantar fasciitis with the highest level of evidence of efficacy (that is, a meta-analysis of multiple, well conducted randomised controlled trials) (Orchard, 2012). However, there are many treatments of low to moderate cost with a lesser degree of supportive evidence. Clinical experience can impart a sense of which treatments are most likely to be useful in which subgroup of individuals (Table 5 above).
In the absence of high quality evidence, it is still possible (and indeed likely) to achieve a high success rate with a combination of the treatments for plantar fasciitis. Allowing a moderately rapid return to ambulation can help address the spiral of immobility causing further weight gain, which contributes to a worsening of the condition, presenting a major challenge in treating many plantar fascia individuals. For this reason, immobilisation (which decreases energy expenditure) is generally a poor choice of treatment for overweight individuals with plantar fasciitis.
The prognosis for most individuals with plantar fasciitis is generally good, particularly if a wide variety of treatment modalities is attempted; although the majority of cases will rsolve with conservative treatment within 3-6 months. With this in mind, the condition should be considered a curable one and every effort made to achieve this, with a high potential secondary gain (in terms of future ability to exercise) if a cure is achieved. However, on a less cheerful not, bilateral and HLA-B27 associated arthritis cases have worst prognosis.
12.0 Summary
- Plantar fasciitis is a condition which generally resolves over time with minimally-invasive management (the occurrence of plantar heel pain commonly signifies a short-lived hindrance for most individuals).
- With a success rate of 85% to 95% when treated early with conservative measures, practitioners should have great optimism in returning athletes and the general population back to their routine activities.
- There is no one treatment with the highest level of evidence, but several with moderate levels of evidence, including stretching, orthotics, shock wave therapy and injections.
- The secondary cost of prolonged immobility can be severe (and can also worsen plantar fasciitis), so it is worth treating plantar fasciitis actively rather than with neglect.
- Choice of treatments should be tailored to the individual’s circumstances and likelihood of response.
- For those without resolution of their pain, a distinction must be made between those with cases resistant to conservative measures from those with potentially incorrect working diagnoses.
- Those in need of surgical intervention will be greatly served by an accurate diagnosis related to specific pathology, allowing more selective decompressions and a faster recovery.
- A return to full activity can reliably be expected by 4 months following adequate physical therapy and sport specific conditioning. Although, individuals should be cautioned that complete recovery may take up to a period of 1 year.
13.0 Further Reading
- Dr Nick Campitelli, a podiatrist based in Akron, OH (USA), specialises in foot and ankle surgery with an interest and enthusiasm for running as well as helping runners with injuries. Visit his blog at: http://www.drnicksrunningblog.com/category/injuries/plantar-fascitis/ for a variety of information relating to plantar fasciitis.
- NICE (National Institute for Health and Clinical Excellence): http://cks.nice.org.uk/plantar-fasciitis updated June 2015.
14.0 References
All references used in the above article can be found in this document: Plantar Fasciitis, An Overview, References for Webpage (2015-07-11)



Hi,
I served in the Canadian Forces for 26 years and 2 years after my release I started to have pain at he bottom of my feet and was disgnosed with plantar fasciitis. I was told that my condition was not related or had nothing to do with my military services at all.
I find that hard to believe after running and wearing combat boots for so many years ,mandatory physical training and section sports that this did not have any effect on my condition.
Could you please give me your comments or any references that I could read on the matter .
Thank you
LikeLike
Hi Mike,
1. Experiencing symptoms of Plantar Fasciitis two years after leaving military service would suggest it is not related to your military service, in my opinion.
2. From my experience, and wisdom in the literature (see Section 4.0 above), cause (of the injury) and effect (i.e. pain and discomfort) are usually close in time (usually a couple of days) – it would be unlikely that the symptoms would manifest after such a long period after the event(s).
3. Have you changed jobs recently (e.g. more standing/walking) or increased/changed the type of training? Your lifestyle since leaving could be a factor.
4. I assume a medical professional (e.g. doctor or physiotherapist) diagnosed your condition?
5. Did you have any lower leg issues during your military service?
6. You can find references in the Word document at the bottom of the webpage.
LikeLike
Thank you very much
Regards
LikeLike
This is an excellent post.
I have been battling with a bunch of lower leg injuries myself, plantar fasciitis, achilles tendonitis etc. Misnomers, I know.
You can see my moans about this subject whilst trying to hike at my own blog here:
http://www.phillipjwellsphotographyblog.wordpress.com
Thanks again for a great article.
Phil
LikeLike
Would plantar fasciitis stop me going in the army? Thanks
LikeLike
Hi Gavin,
Short Answer: Maybe
Longer Answer: It would (most likely) depend on the cause. For example, if caused by over-training, then fairly transient in nature. However, if caused by a pronated foot type then longer term issues occur (if not able to treat with special insoles (orthoses)). Remember the MOD medical examiner has the final decision; your own doctor may give a different prognosis.
If you want a more specific answer I would require more info about your plantar fasciitis.
LikeLike