
Introduction
Do you know what a Lisfranc injury is, or even where your Lisfranc ligament is? If the answer is no then reading this article will provide you with a basic insight to Lisfranc injuries.
What Are Lisfranc Injuries?
A Lisfranc injury is a disruption of the tarsometatarsal ligamentous joint complex in the foot. The key anatomical structure is the Lisfranc ligament, an interosseous ligament spanning the medial cuneiform and the base of the second metatarsal that provides most of the stability to the joint complex. Disruption usually results in displacement of the joint, most commonly of the second, third, or first tarsometatarsal articulations. A Lisfranc injury can result from isolated tarsometatarsal ligamentous disruption, osseous disruption, or a combination of both.
Lisfranc injuries occur by both high energy mechanisms such as motor vehicle collisions and low energy mechanisms such as tripping or landing awkwardly during recreational sports. Although the injury can occur after a direct dorsal blow to the foot, it is more commonly a consequence of axially loading the foot from the back of the heel while the ankle is plantar flexed and the forefoot is on the ground, causing the mid-foot to buckle dorsally (Myerson & Cerrato, 2008).
How Common Are Lisfranc Injuries?
Although Lisfranc injuries are reported to represent 0.2% of orthopaedic injuries (Sands & Grose, 2004), the actual incidence is probably higher because they are often misdiagnosed. A recent literature review by van Rijn et al. (2011) found that Lisfranc injuries are missed on initial presentation in one third of cases.
These injuries often accompany tarsal or metatarsal fractures, which comprise 6% of all fractures in the primary care setting (Hatch & Rosenbaum, 1994). Certain subgroups have an increased risk of Lisfranc injuries – for example, the incidence is 4% among collegiate American football players (Meyer et al., 1994).
Why Are Lisfranc Injuries Missed?
Although Lisfranc injuries are often associated with high energy trauma, up to one third occur by low energy mechanisms (Vuori & Aro, 1993), and these are more likely to be misdiagnosed (Englanoff et al., 1995; van Rijn et al., 2011). Commentators (Kaplan et al., 1991; Sherief et al., 2007) suggest that this is because the subtle radiographic displacements are easily missed and it is also common for them to be overlooked when patients have multiple injuries.
Why Does This Matter?
Without prompt diagnosis and intervention, Lisfranc injuries can lead to tarsometatarsal instability, pain, and post-traumatic mid-foot arthritis. The articular contact area of the joint is significantly diminished with as little as 3 mm of displacement, which causes increased joint pressures and subsequent cartilage degeneration (Ebraheim et al., 1996).
How Are Lisfranc Injuries Diagnosed?
Clinically
Accurate diagnosis of Lisfranc injuries requires a high index of suspicion. Patients present with tenderness or swelling over the dorsal-medial tarsometatarsal joint complex and are unable to bear weight on the affected foot. The presence of ecchymosis[1] over the plantar mid-foot should raise clinical suspicion of Lisfranc injury. With more severe disruption of the tarsometatarsal joint, plantar or dorsal bony malalignment of the metatarsal is palpable.
Investigations
Non-weight bearing radiographs may appear normal in up to half of patients with proved Lisfranc disruption (Nunley & Vertullo, 2002). Weight bearing foot radiographs (anteroposterior, lateral, and 30° oblique views) should be obtained in any patient with a suspected Lisfranc injury if initial non-weight bearing radiographs appear normal. Diastasis or displacement of the second metatarsal-medial cuneiform space is diagnostic of disruption of the Lisfranc joint complex (Potter et al., 1998).
In weight bearing anteroposterior radiographs, the medial border of the second metatarsal base should be co-linear with the medial border of the intermediate cuneiform when the joint is uninjured (figure 2). In some cases, malalignment is obvious in the radiography (figure 3). Adequate anteroposterior radiographs must show a tangential view of the second tarsometatarsal joint (figure 1, right) since views oblique to the joint may miss subtle displacements (figure 1, middle). Radiographs may show a small bony avulsion type fracture between the first and second tarsometatarsal joints (figure 3, left) (Myerson et al., 1986).
If weight bearing radiographs show no abnormality and clinical suspicion remains high, computed tomography or magnetic resonance imaging is indicated (Potter et al., 1998). A weight bearing radiograph of the non-injured leg may also be useful for comparison when diagnosing subtle Lisfranc injuries.
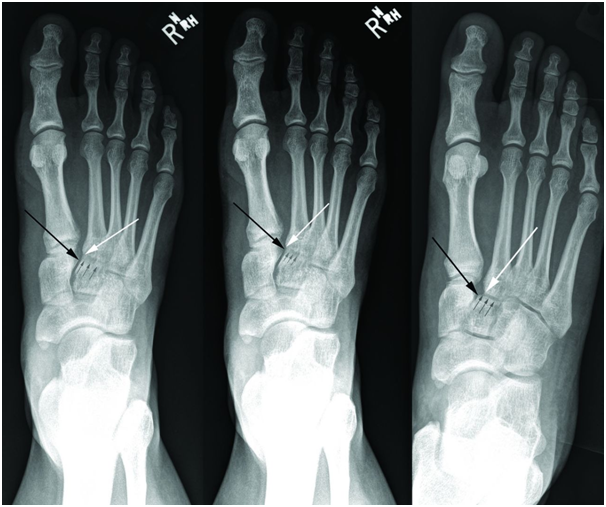
Figure 1: Radiographs showing the importance of obtaining the correct positioning to detect a subtle disruption of the Lisfranc joint. The white arrow indicates the medial base of the second metatarsal, the black arrow the proximal medial corner of the intermediate cuneiform, and the small grey arrows where the second tarsometatarsal joint line should be seen. Left: Anteroposterior radiograph of non-weight bearing right foot shows normal anatomical midfoot alignment in a patient with a Lisfranc injury. Note that the second tarsometatarsal joint line is not visible, indicating that the radiograph is not a true anteroposterior view. Middle: Anteroposterior weight bearing radiograph shows no widening of the medial tarsal-second metatarsal space. Again, the second tarsometatarsal joint line is not visible because of incorrect positioning of the x ray beam. Right: Weight bearing radiograph of the same patient with the correct x ray projection. The lateral shift of the second tarsometatarsal joint indicates disruption of the Lisfranc ligament.

Figure 2: Radiograph of a normal Lisfranc joint. The line of small grey arrows indicates the second tarsometatarsal joint line. The medial base of the second metatarsal (white arrow) and the medial aspect of the intermediate cuneiform (black arrow) line up exactly.

Figure 3: Widely displaced Lisfranc injury. Left: Anteroposterior view showing lateral displacement of the Lisfranc articulations. Right: Lateral view showing the dorsal displacement of the metatarsals (white arrow) relative to the mid-foot (black arrow).
How Are They Managed?
Anatomical reduction of the Lisfranc joint complex is required to prevent subsequent mid-foot arthritis. In displaced injuries, this requires surgical reduction and stabilisation. Acutely, patients with Lisfranc injuries should have their foot splinted and kept non-weight bearing and be referred to an orthopaedic surgeon for ongoing treatment.
Facebook Community, Support & Further Information
This page (see link) provides information and links for those who have had a Lisfranc (foot) injury – with or without associated fractures and/or dislocations: https://www.facebook.com/LisfrancFractureClub
Notes
[1] Ecchymosis is the escape of blood into the tissues from ruptured blood vessels marked by a livid black-and-blue or purple spot or area.
References
Ebraheim, N.A., Yang, H., Lu, J. & Biyani, A. (1996) Computer Evaluation of Second Tarsometatarsal Joint Dislocation. Foot and Ankle International. 17(11), pp.685-689.
Engelanoff, G., Anglin, D. & Hutson, H.R. (1995) Lisfranc Fracture-dislocation: A Frequently Missed Diagnosis in the Emergency Department. Annals of Emergency Medicine. 26(2), pp.229-233.
Hatch, R.L. & Rosenbaum, C.L. (1994) Fracture Care by Family Physicians: A Review of 295 Cases. Journal of Family Practice. 38(3), pp.238-244.
Kaplan, J.D., Karlin, J.M., Scurran, B.L. & Daly, N. (1991) Lisfranc’s Fracture-dislocation: A Review of the Literature and Case Reports. Journal of the American Podiatric Medical Association. 81(10), pp.531-539.
Meyer, S.A., Callaghan, J.J., Albright, J.P., Crowley, E.T. & Powell, J.W. (1994) Midfoot Sprains in Collegiate Football Players. American Journal of Sport Medicine. 22(3), pp.392-401.
Myerson, M.S. & Cerrato, R.A. (2008) Current Management of Tarsometatarsal Injuries in the Athlete. Journal of Bone and Joint Surgery of America. 90, pp.2522-2533.
Myerson, M.S., Fisher, R.T., Burges, A.R. & Kenzora, J.E. (1986) Fracture Dislocations of the Tarsometatarsal Joints: End Results Correlated with Pathology and Treatment. Foot and Ankle. 6(5), pp.225-242.
Nunley, J.A. & Vertullo, C.J. (2002) Classification, Investigation, and Management of Midfoot Sprains: Lisfranc Injuries in the Athlete. American Journal of Sports Medicine. 30(6), pp.871-878.
Potter, H.G., Deland, J.T., Gusmer, P.B., Carson, E. & Warren, R.F. (1998) Magnetic Resonance Imaging of the Lisfranc Ligament of the Foot. Foot and Ankle International. 19(7), pp.438-446.
Sands, A.K. & Grose, A. (2004) Lisfranc Injuries. Injury. 35(2) Supplement, pp.71-76.
Sherief, T.I., Mucci, B. & Greiss, M. (2007) Lisfranc Injury: How Frequently Does It Get Missed? And How Can We Improve? Injury. 38(7), pp.856-860.
Van Rijn, J., Dorleijn, D.M., Boetes, B., Wiersma-Tuinstra, S. & Moonen, S. (2012) Missing the Lisfranc Fracture: A Case Report and Review of the Literature. Journal of Foot and Ankle Surgery. 51(2), pp.270-274.
Vuori, J.P. & Aro, H.T. (1993) Lisfranc Joint Injuries: Trauma Mechanisms and Associated Injuries. Journal of Trauma. 35(1), pp.40-45.


